
Take a deep breath in and hold it Try to take another deep breath in on top of the previous breath Aim to take another 1-3 breaths in the same way 3-5 breaths in total Breathe out or cough Repeat this process 3-5 times How often should I do it. Proportional modes improve patient-ventilator coupling resulting in greater comfort and less dyspnea but not in improved outcomes with respect to the duration of mechanical ventilation delirium or cognitive impairment.
Mechanical Ventilation From Bench To The Bedside Review Recapem
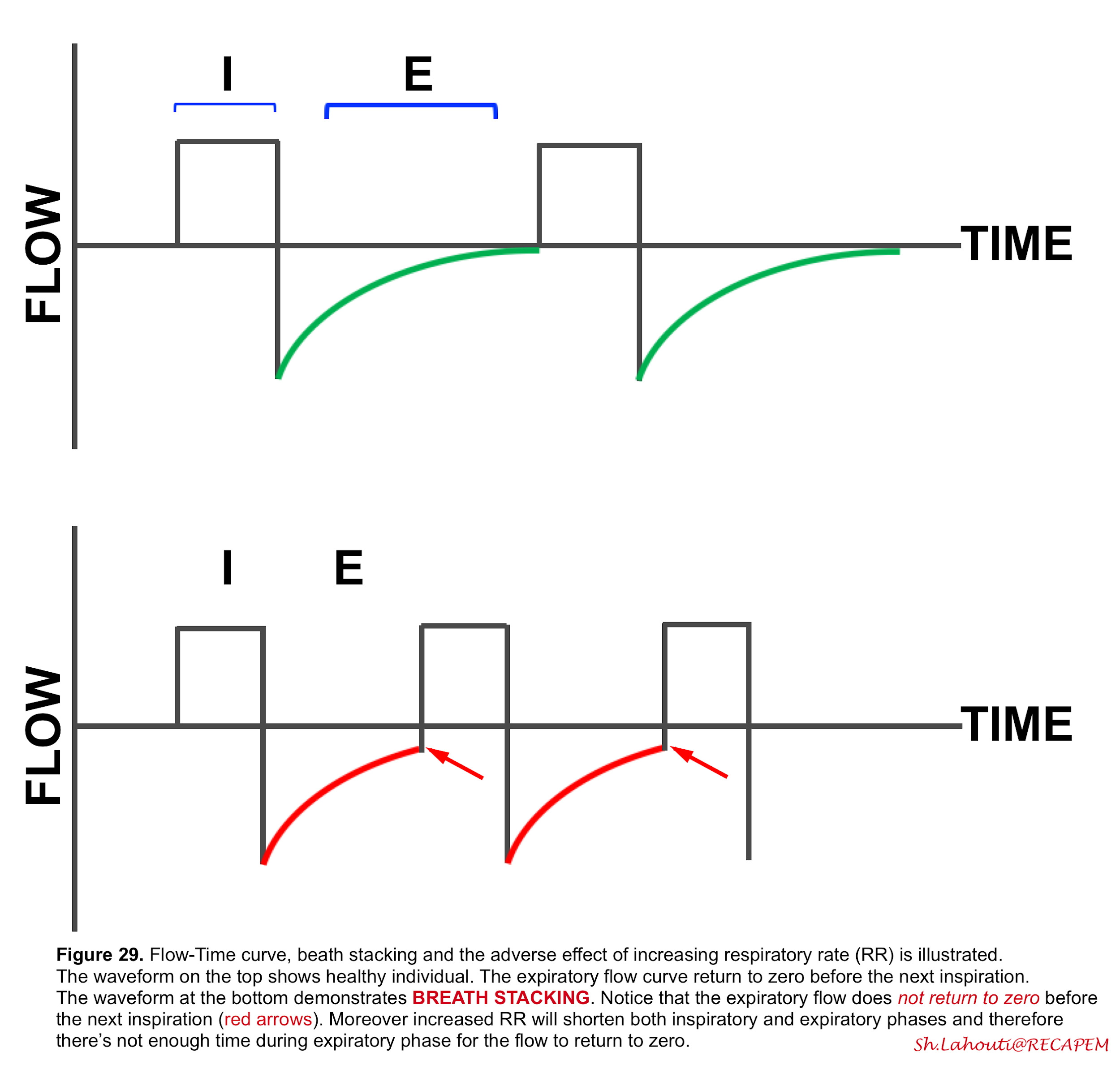
So increasing the tidal volume or respiratory rate could actually reduce the minute ventilation because of the breath stacking potential.
How to fix breath stacking on vent. Specifically the mechanical breath I. Excessive tidal volume from breath stacking during. Time sec Airway Pressure cm H 2 O.
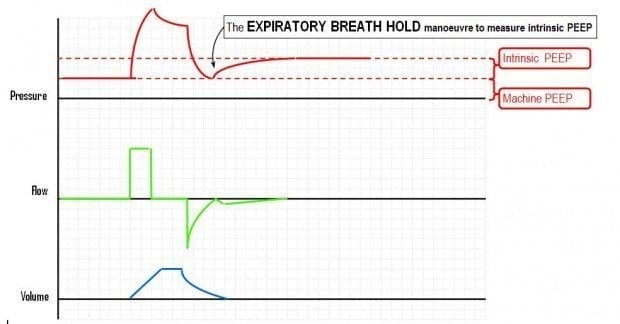
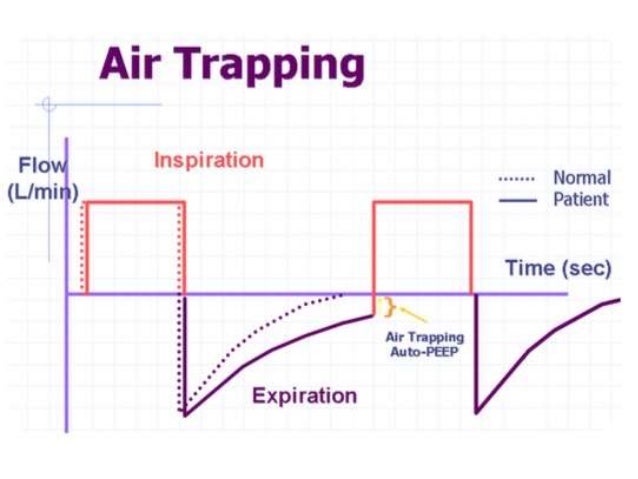
Acute causes of elevated elastic work are pneumothorax tension pneumothorax evolving pneumonia pulmonary edema ARDS and auto-PEEP caused by breath stacking. Plateau pressures greater than 30 cmH20 have been implicated in ventilator-induced lung injury VILI. How to fix it.
PS is usually added to aid in comfort and increase the patients spontaneous Vt. Stacked breaths occur frequently in low tidal volume ventilation despite deep sedation and result in volumes substantially above the set tidal volume. Compared with increasing sedation-analgesia adapting the ventilator to patient breathing effort reduces breath-stacking asynchrony significantly and often dramatically.
If the patient breathes at the time the ventilator is due to give a set breath the ventilator will synchronize with the patients breath. External PEEP which is greater than the pressure level in upstream airways will reduce work of breathing by opening these airways for the patient. Clinicians progressively learned how to detect asynchronies visually by looking at ventilator waveforms at the bedside and how to adapt ventilator settings accordingly breath by breath.
Breath dyssynchrony stacking BDS refers to the unintended high tidal volumes that occur as a consequence of incomplete exhalation between consecutive inspiratory cycles delivered by the ventilator. Provide High Flow Oxygen with PEEP Valve if needed High peak pressure alone cannot distinguish cause. Better Breath-Stacking Index Improvement through Ventilator Setting Effective measures.
Current evidence suggests that the best approach to managing asynchronies is by adjusting ventilator settings. If problem cannot easily be detected. Set tidal volume has a strong influence on frequency of stacked breaths.
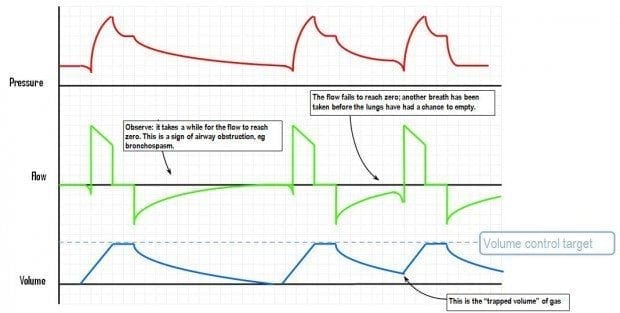
This can commonly occur during volume-preset assist control modes during lung protective ventilation for ARDS. Asynchrony in each breath phase -Triggering -Flow demand. In volume control mode of ventilation when the inspiratory time Ti of the patient is greater than the Ti of the ventilator or respirator the patient cont.
However if the patient triggers the ventilator at a rate greater than the set rate these two strategies diverge. High minute ventilation high lung compliance high expiratory resistance due to airway or circuit all reduce expiration time and flow resulting in auto. If they are on a ventilator you can see it as the volume getting progressively higher with each breath and the patient not completing a full expiration before trying to inspire again.
The most common causes for DT are the improper matching of mechanical breath I-times to neural I-times and an insufficient level of pressure support with high respiratory drives 7. Usually occurs when patient is breathing out of synced with ventilator settings coughing or other negative stimulation can do this as well. Plateau pressure must be obtained.
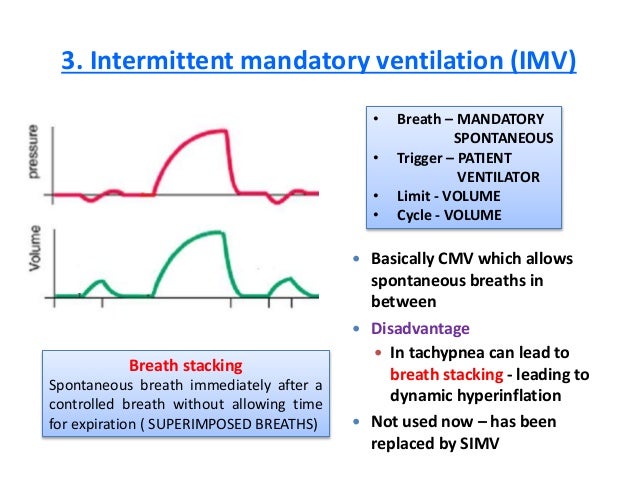
CPAP means continuous positive airway pressure. In between the mandatory breaths the patient can breathe on hisher own. Set tidal volume has a strong influence on frequency of stacked breaths.
Increase in respiratory drive andor insufficient ventilator assistance Despite the delivery of a breath by the ventilator when the patients demand is high the inspiratory effort may continue throughout the preset ventilator inspiratory time and remains present after. In addition they realized that the time required for such management was not compatible with everyday clinical practice in the ICU. The air from the previous breath has not been exhaled fully before the next breath so breaths start to stack on top of one another.
2-3 times a day but can be completed more often if. Provide bag-valve-mask PPV while troubleshooting. In AC each breath above the set respira-tory rate will result in a full mechanically supported breath at the set tidal volume.
In SIMV the ventilator will only give the set number of breaths. These results support an algorithm beginning with ventilator adjustment to rationalize the management of severe breath-stacking as.
Https Www Draeger Com Library Content 6 Weaning Process Pdf
Https Www Draeger Com Library Content 6 Weaning Process Pdf
Ventilator Breath Stacking Arrows Occurs When A Mandatory Breath Is Download Scientific Diagram

Double Triggering Diagnosis Differentiation And Resolution
Intrinsic Peep Litfl Ccc Ventilation
Patient Ventilator Dyssynchrony Deranged Physiology


Short Cycling
Intrinsic Peep Litfl Ccc Ventilation

Double Triggering Diagnosis Differentiation And Resolution

Mechanical Ventilation Waveform Analysis Youtube
Mechanical Ventilation Basics
![]()
Ventilator Breath Stacking Arrows Occurs When A Mandatory Breath Is Download Scientific Diagram
![]()
Ventilator Breath Stacking Arrows Occurs When A Mandatory Breath Is Download Scientific Diagram

Reverse Triggering
![]()
Ventilator Breath Stacking Arrows Occurs When A Mandatory Breath Is Download Scientific Diagram

Ventilator Breath Stacking Arrows Occurs When A Mandatory Breath Is Download Scientific Diagram

Double Triggering Diagnosis Differentiation And Resolution
![]()
Double Triggering Arrow Is The Result Of The Ventilator Inspiratory Download Scientific Diagram
Conv Ventilation Physi